Medically reviewed and approved by a board-certified member
Hemotology
RED CELLS MORPHOLOGY
By Dayyal Dg.Twitter Profile | Updated: Sunday, 06 August 2017 07:12 UTC
 Red cells are best examined in an area where they are just touching one another (towards the tail of the film). Normal red cells are 7-8 μm in size, round with smooth contours, and stain deep pink at the periphery and paler in the center. Area of central pallor is about 1/3rd the diameter of the red cell. Size of a normal red cell corresponds roughly with the size of the nucleus of a small lymphocyte. Normal red cells are described as normocytic (of normal size) and normochromic (with normal staining intensity i.e. hemoglobin content).
Red cells are best examined in an area where they are just touching one another (towards the tail of the film). Normal red cells are 7-8 μm in size, round with smooth contours, and stain deep pink at the periphery and paler in the center. Area of central pallor is about 1/3rd the diameter of the red cell. Size of a normal red cell corresponds roughly with the size of the nucleus of a small lymphocyte. Normal red cells are described as normocytic (of normal size) and normochromic (with normal staining intensity i.e. hemoglobin content).Morphologic abnormalities of red cells in peripheral blood smear can be grouped as follows:
- Red cells with abnormal size (see Figure 799.1)
- Red cells with abnormal staining
- Red cells with abnormal shape (see Figure 799.1)
- Red cell inclusions (see Figure 799.2)
- Immature red cells (see Figure799.3)
- Abnormal red cell arrangement(see Figure 799.4).
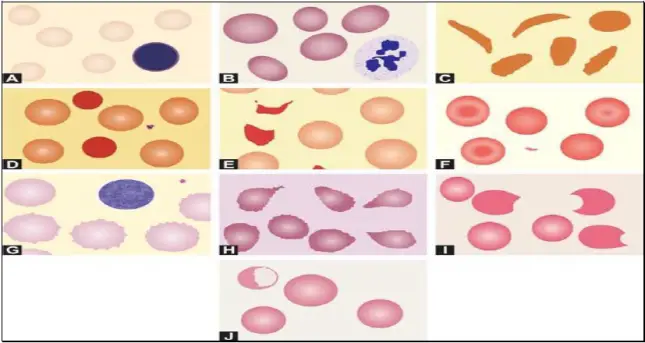
Red cells with abnormal size:
Mild variation in red cell size is normal. Increased variation in red cell size is called as anisocytosis. This is a feature of most anemias and is non-specific. Anisocytosis is due to the presence of microcytes, macrocytes, or both in addition to red cells of normal size.
Microcytes are red cells smaller in size than normal. They are seen when hemoglobin synthesis is defective i.e. in iron deficiency anemia, thalassemias, anemia of chronic disease, and sideroblastic anemia.
Macrocytes are red cells larger in size than normal. Oval macrocytes (macro-ovalocytes) are seen in megaloblastic anemia, myelodysplastic syndrome, and in patients being treated with cancer chemotherapy. Round macrocytes are seen in liver disease, alcoholism, and hypothyroidism.
Red cells with abnormal staining (hemoglobin content):
Staining intensity of red cells depends on hemoglobin content. Red cells with increased area of central pallor (i.e. containing less hemoglobin) are called as hypochromic. They are seen when hemoglobin synthesis is defective, i.e. in iron deficiency, thalassemias, anaemia of chronic disease, and sideroblastic anemia.
In dimorphic anemia, there are two distinct populations of red cells in the same smear. An example is presence of both normochromic and hypochromic red cells seen in sideroblastic anemia, iron deficiency anemia responding to treatment, and following blood transfusion in a patient of hypochromic anemia. In myelodysplastic syndrome, dimorphic picture results from admixture of microcytic hypochromic cells and macrocytes.
Red cells with abnormal shape:
Increased variation in red cell shape is called as poikilocytosis and is a feature of many anemias. A red cell that is abnormal in shape is called as a poikilocyte.
Sickle cells are narrow and elongated red cells with one or both ends pointed. Sickle form is assumed when a red cell containing hemoglobin S is deprived of oxygen. Sickle cells are seen in sickle cell disorders, particularly sickle cell anemia. Sickle cells are not seen on blood smear in neonates with sickle cell disease because high percentage of fetal hemoglobin in red cells prevents sickling.
Spherocytes are red cells, which are slightly smaller in size than normal, round, stain intensely, and do not have central area of pallor. The surface area of spherocytes is less as compared to the volume. They are seen in hereditary spherocytosis, autoimmune hemolytic anemia (warm antibody type), and ABO hemolytic disease of newborn.
Schistocytes are fragmented red cells, which take various forms like helmet, crescent, triangle, etc. and usually have surface projections or spicules. They are seen in microangiopathic hemolytic anemia, cardiac valve prosthesis, and severe burns.
Target cells are red cells with bull's eye appearance. These red cells show a central stained area and a peripheral stained rim with unstained cytoplasm in between. They are seen in hemoglobinopathies (e.g. thalassemias, hemoglobin disease, sickle cell disease), obstructive jaundice, and following splenectomy.disease, sickle cell disease), obstructive jaundice, and following splenectomy.
Burr cells or echinocytes are small red cells with regularly placed small projections on surface. They are seen in uremia.
Acanthocytes are red cells with irregularly spaced sharp projections of variable length on surface. They are seen in spur cell anemia of liver disease, McLeod phenotype, and following splenectomy.
Teardrop cells or dacryocytes have a tapering droplike shape. Numerous teardrop red cells are seen in myelofibrosis and myelophthisic anemia.
Blister cells or hemi ghost cells are irregularly contracted cells in which hemoglobin is contracted and condensed away from the cell membrane. This is seen in glucose-6-phosphate dehydrogenase defici-ency during acute hemolytic episode.
Bite cells result from removal of Heinz bodies by the pitting action of the spleen (i.e. a part of red cell is bitten off by the splenic macrophages). They are seen in glucose-6-phosphate dehydrogena-se deficiency and unstable hemoglobin disease.
Red cell inclusions:
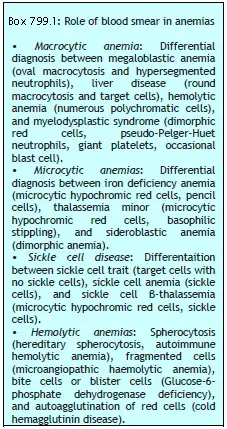
Those inclusions that can be visualized on Romanowsky-stained smears are basophilic stippling, Howell-Jolly bodies, Pappenheimer bodies, and Cabot's rings.
Basophilic stippling or punctate basophilia refers to the presence of numerous, irregular basophilic (purple-blue) granules which are uniformly distributed in the red cell. These granules represent aggregates of ribosomes. Their presence is indicative of impaired erythropoiesis and they are seen in thalassemias, megaloblastic anemia, heavy metal poisoning (e.g. lead), and liver disease.cell. These granules represent aggregates of ribosomes. Their presence is indicative of impaired erythropoiesis and they are seen in thalassemias, megaloblastic anemia, heavy metal poisoning (e.g. lead), and liver disease.
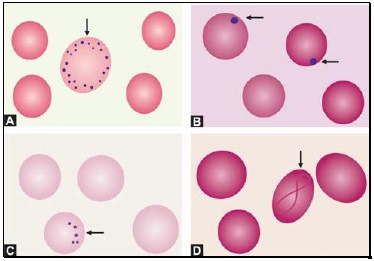
Figure 799.2 Red cell inclusions: (A) Basophilic stippling; (B) Howell-Jolly bodies; (C) Pappenheimer bodies; (D) Cabot’s ring
Howell-Jolly bodies are small, round, purple-staining nuclear remnants located peripherally in red cells. They are seen in megaloblastic anemia, thalasse-mias, hemolytic anemia, and following splenectomy.
Pappenheimer bodies are basophilic, small, ironcontaining granules in red cells. They give positive Perl's Prussian blue reaction. Unlike basophilic stippling, Pappenheimer bodies are few in number and are not distributed throughout the red cell. They are seen following splenectomy and in thalassemias and sideroblastic anemia.
Cabot's rings are fine, reddish-purple or red, ring-like structures. They appear like loops or figure of eight structures. They indicate impaired erythropoiesis and are seen in megaloblastic anemia and lead poisoning.
Immature red cells:
Polychromatic cells are young red cells containing remnants of ribonucleic acid. These cells are slightly larger than normal red cells and have a diffuse bluishgrey tint. (They represent reticulocytes when stained with a supravital stain like new methylene blue). Polychromasia is due to the uptake of acid stain by hemoglobin and basic stain by ribonucleic acid. Presence of polychromatic cells is indicative of active erythropoiesis and are increased in hemolytic anemia, acute blood loss, and following specific therapy for nutritional anemia.and are increased in hemolytic anemia, acute blood loss, and following specific therapy for nutritional anemia.
Nucleated red cells are red cell precursors (erythroblasts), which are released prematurely in peripheral blood from the bone marrow. They are a normal finding in cord blood of newborns. Large number of nucleated red cells in blood smear is seen in hemolytic disease of newborn, hemolytic anemia, leukemias, myelophthisic anemia, and myelofibrosis.
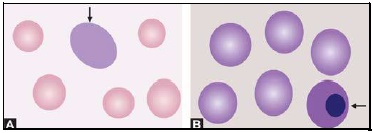
Figure 799.3 Immature red cells: (A) Polychromatic red cell; (B) Nucleated red cell
Abnormal red cell arrangement:
Rouleaux formation refers to alignment of red cells on top of each other like a stack of coins. It occurs in multiple myeloma, Waldenström's macroglobulinemia, hypergammaglobulinemia, and hyper fibrinogenemia.
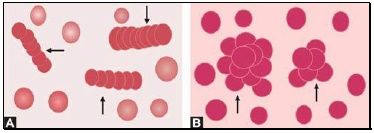
Figure 799.4 Abnormal red cell arrangement: (A) Rouleaux formation; (B) Autoagglutination
Autoagglutination refers to the clumping of red cells in large, irregular groups on blood smear. It is seen in cold agglutinin disease. Role of blood smear in anemia is shown in Box 799.1 and Figures 799.5 to 799.7.
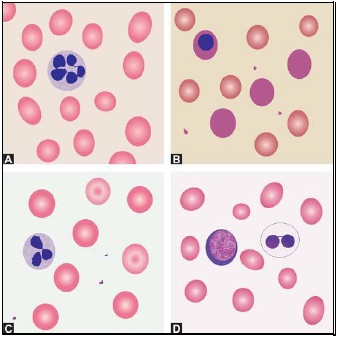
Figure 799.5 Differential diagnosis of macrocytic anemia on blood smear: (A) Megaloblastic anemia; (B) Hemolytic anemia; (C) Liver disease; (D) Myelodysplastic syndrome
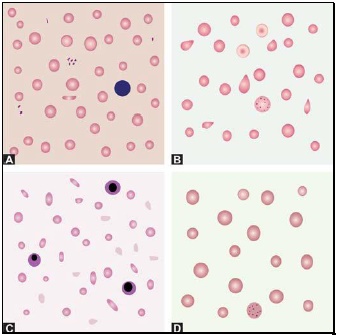
Figure 799.6 Differential diagnosis of microcytic anemia on blood smear: (A) Iron deficiency anemia; (B) Thalassemia minor; (C) Thalassemia major; (D) Sideroblastic anemia
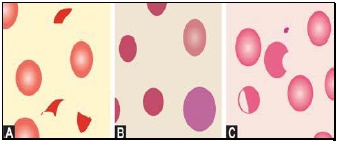
Figure 799.7 Differential diagnosis of hemolytic anemia on blood smear. (A) Microangiopathic hemolytic anemia showing fragmented red cells, (B) Hereditary spherocytosis showing spherocytes and a polychromatic red cell, and (C) Glucose-6-phosphate dehydrogenase deficiency showing a blister cell and a bite cell
Further Reading:
- Comment
- Posted by Dayyal Dg.
Tags:
End of the article